How one inherited signal can amplify more than one heart risk pathway.
This atlas shows how high Lipoprotein(a) [Lp(a)] can sit upstream of artery, valve, and family risk pathways. Use the slider to move from inherited signal to lifelong exposure, artery amplification, valve amplification, and compounded risk context.
Common and inherited
Why Lp(a) needs its own risk map
Lp(a) matters because it is both common and largely inherited. These two facts change the conversation: one result can clarify risk for one person, and may also point relatives toward testing.
Common
Roughly 1 in 5 people have elevated Lp(a).
This makes high Lp(a) common, even though many people have never heard of it, and standard cholesterol checks do not include it.
High Lp(a) can increase risk because:
The level matters. Almost everyone has some Lp(a); the risk comes from having elevated levels.
Lp(a) is less familiar than HDL or LDL. Many people know about “good” and “bad” cholesterol, but few have heard of “stealth” cholesterol.
Lifestyle matters. Even if it does not directly lower Lp(a), lifestyle can reduce other risks around it.
New treatment trials are underway. Several Lp(a)-targeting medicines are being tested, including gene-silencing therapies.
It can be part of a complicated risk picture. Insulin resistance and metabolic risk, for example, can make Lp(a) numbers and interpretation more challenging.
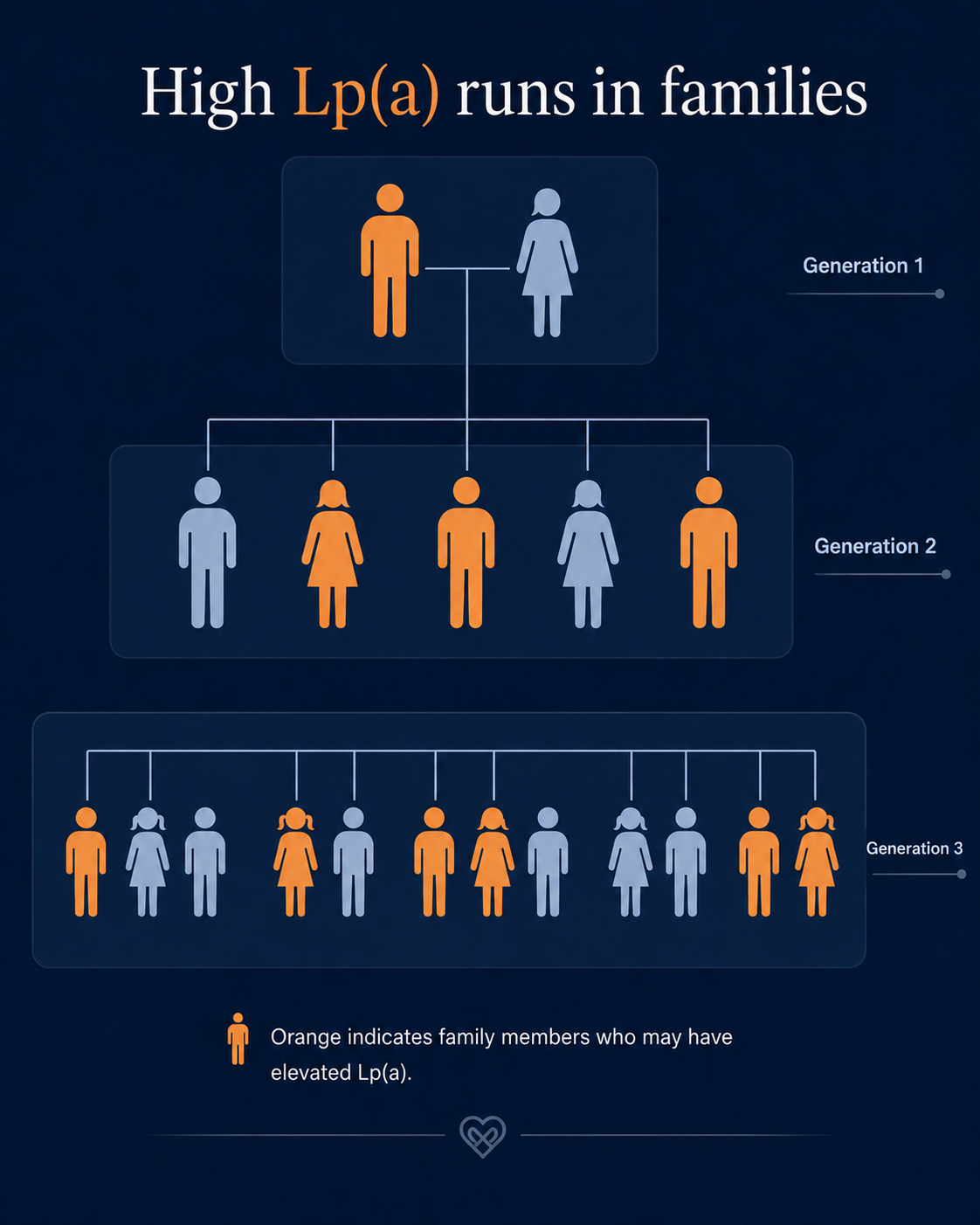
Inherited
Lp(a) can run through families.
If one person has high Lp(a), close relatives may also need testing. The highlight shows possible family relevance, not certainty for every relative.
1
Test once. Lp(a) is inherited, so one test can clarify your lifelong risk signal. But a low number does not always mean all clear. In insulin resistance or high-insulin states, Lp(a) may be "masked" and appear low, which is why any result needs wider risk context.
2
Build your risk picture. Your risk is easier to understand when Lp(a) is read alongside ApoB, blood pressure, metabolic risk, inflammation, imaging, and family history details.
3
Have informed conversations. Your result may help your parents, siblings, children, and other people you love consider whether to get tested, and help you make better decisions with your health team.
Lp(a) risk pathway visualisation
Amplifier view reveals risk-layer chips, family links, and module hand-offs. It does not estimate your personal risk.
Lp(a) is a cholesterol-carrying particle whose level is mostly determined by genetics. Many people with high Lp(a) have no symptoms.
It can be hidden
A standard cholesterol panel does not include Lp(a). The only way to know your level is to get a test.
It connects artery and valve pathways
Elevated Lp(a) contributes to artery disease — plaque, inflammation, rupture, clot, heart attack, stroke, and to valve disease — aortic valve calcification and aortic stenosis. Few risk factors are so clearly linked to both pathways.
Lifestyle still matters
Lifestyle does not lower Lp(a), but it can reduce overall cardiovascular risk. This understanding is important and can be empowering by taking the right actions.
Family testing matters
Because Lp(a) is inherited, a high result may be relevant to close relatives. Cascade testing can help families find hidden risk earlier.
Specific therapies are emerging
Several Lp(a)-targeting therapies are in clinical trials, including gene-silencing approaches, but none are yet in routine clinical use. If Lp(a) poses a risk for you or loved one, ask your health team about the current state of Lp(a) treatment options.
Normal LDL does not rule out high Lp(a)
Lp(a) can be high even when standard cholesterol results look acceptable. That is why a separate Lp(a) measurement matters.
High Lp(a) is not destiny
A high Lp(a) result does not mean a heart attack, stroke, or valve damage is inevitable. It means this hidden risk should be made visible and managed deliberately.
Do not wait for symptoms
Lp(a) does not announce itself. Testing is about finding this inherited risk before cardiovascular damage or an event reveals it.
Heart risk products
Clarify risk. Navigate danger. Prevent events.
High Lp(a) is rarely a single-answer problem. The practical question is how it fits with your current tests, family history, artery risk, valve risk, and modifiable risk layers. Start with Clarify if you need to organise what your checks show and miss. Use Navigate if you already have signals to connect. Use Prevent if you want a structured plan to reduce avoidable cardiovascular damage.